Demo Topic: Diagnostic Pacing
The concept of electrophysiology was first recognised in the 1960’s, followed by diagnostic simulation in the 1970’s and finally RFA in the 1980’s (Boyle, 2002). This section explains the main protocols and their uses: to induce, to measure, or to terminate a tachycardia.
From this point forward it is assumed that all students are familiar with the common pacing terminology explained in Pacing 1 – Fundamentals (such as “S1”, burst, BPM conversion to milliseconds, etc).
4. Terminating arrhythmias
Re-entrant Arrhythmia termination
Termination of arrhythmias by pacing aims to capture part of the circuit during it excitable phase, and render it refractory to the tachycardia wavefront.
Method 1: Overdrive burst pace (also valid for triggered arrhythmias)
Burst pacing is similar to standard pacing, but implies a rapid short lived period of pacing in S1. It delivers S1 pacing at specified cycle length. Usually only 5-10 seconds of pacing is required. Rarely up to 30 seconds of pacing may be needed (e.g. to overdrive atrial flutter).
Overdrive pacing requires an S1 pacing train delivered at faster rate than the TCL (normally it is used the formula 90% TCL, which usually means 50ms or faster), for about 10 beats. As this may transiently entrain the tachycardia, it may allow continuation of the tachycardia, so multiple attempts may be required.
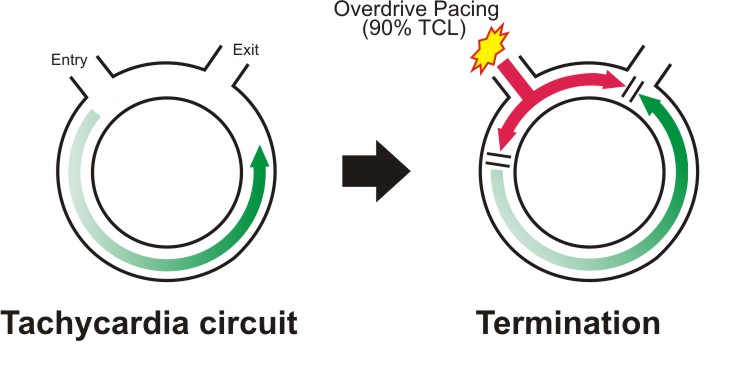
Above, Overdrive suppression phenomenon in re-entrant tachycardias.

Method 2: Underdrive pace
Underdrive pacing uses a fixed S1 train significantly slower than the tachycardia, so must be delivered in asynchronous mode (A00 or V00), and relies on the chance delivery of an asynchronous pacing beat into an excitable gap in the tachycardia, which then interrupts the tachycardia.
There is a potential risk that due to pacing into the tachycardia, that pacing may occur on a vulnerable part of the T wave and VF be induced. However in a highly monitored environment such as an EP lab, this risk is very small.

![]() A very interesting article: "Underdrive pacing to terminate ventricular tachycardia" by Richard Bond, Paul W X Foley, Yaver Bashir.
A very interesting article: "Underdrive pacing to terminate ventricular tachycardia" by Richard Bond, Paul W X Foley, Yaver Bashir.
Method 3: Sensed extras – single or multiple
Single Extra stimuli can also be used to render part of the tachycardia circuit refractory, similar to underdrive pacing, but uses synchronised impulses.
The initial impulse should be delivered just shorter than the TCL, and then progressively shortened or “scanned” until the tachycardia terminates (or extra-stimulus becomes refractory). Once successfully terminated, a single extra-stimulus to the same site at the same coupling interval can then be used to rapidly terminate the same tachycardia without the need for “scanning extras”.
Decremental pacing during SVT
This is not frequently used. If during an antegrade study, an SVT is initiated, once adequate pacing maneuvers have been performed to identify the tachycardia, rather than burst pacing to terminate the tachycardia, an AV wenckebach test can be performed, starting at TCL, and terminating when AV block occurs in the usual manner. This can save the need to start an AVW test from sinus cycle lengths.